
Are you struggling with relentless hip pain that limits your daily activities and diminishes your quality of life? At Dr. Alexander McLawhorn's practice in NYC and Stamford, CT, we can help you reclaim your mobility and get back to the activities you love.
With a total hip replacement, we aim to restore your hip function and improve your overall well-being. Discover how this surgical procedure can transform your life and why patients trust Dr. McLawhorn for their hip care needs.
What Is Total Hip Replacement?
Total hip replacement, also known as total hip arthroplasty, is a surgical reconstruction of the hip joint using prosthetic parts made of special metals, plastic, and/or ceramics. Total hip replacement surgery is commonly performed to repair a hip joint suffering from damaged cartilage and/or bone, usually due to hip arthritis.
Why Is Total Hip Replacement Surgery Performed?
Total hip replacement surgery is generally performed when there is substantial damage to the cartilage or bone in the hip joint and when a patient is suffering from a lot of pain. The surgery eliminates the pain associated with these conditions and restores function and mobility to the hip joint. In addition to hip arthritis, total hip replacement may be performed for avascular necrosis (bone death of the femoral head, or ball, of the joint) and other congenital and acquired hip disorders. Occasionally, total hip replacement is the right treatment for hip impingement when there’s severe damage to the hip cartilage.

What Are the Goals for Total Hip Replacement Surgery?
First and foremost, total hip replacement surgery aims to improve pain. Other general goals are:
- Improve hip function
- Provide a stable hip that does not dislocate
- Prevent excessive wear of the implanted components
- Avoid complications
Ideally, patients can return to work and the activities they love to perform without worrying about their hip replacement. After complete recovery from surgery, some patients may even forget that they had a hip replacement.
Why Choose Dr. McLawhorn at the Hospital for Special Surgery (HSS)?

Dr. Alexander McLawhorn is a top orthopedic surgeon specializing in hip replacement surgery. He uses advanced techniques to ensure less pain and a faster recovery. He provides care at one of the nation’s leading orthopedic institutions, the Hospital for Special Surgery (HSS), known for its exceptional patient outcomes and innovative treatments.
Dr. McLawhorn works with a dedicated team of board-certified physician assistants to offer personalized care tailored to your needs. You'll receive comprehensive support from your first consultation to post-surgery follow-ups to ensure a smooth and successful recovery. Trust Dr. McLawhorn and his team at HSS to help you regain mobility and live pain-free.
What Does Total Hip Replacement Surgery Involve?
We’ll customize your total hip replacement procedure depending on your needs. That means the specific steps of the surgery can vary from person to person. However, in most cases, you can expect the following:
- We'll provide regional anesthesia with either a spinal or epidural to numb your body from the waist down, and sedation through an IV will allow you to sleep throughout the surgery. We'll also give you antibiotics before the surgery to prevent infection.
- Dr. McLawhorn will access the hip joint either from the front (anterior) or back (posterior) aspect of the joint.
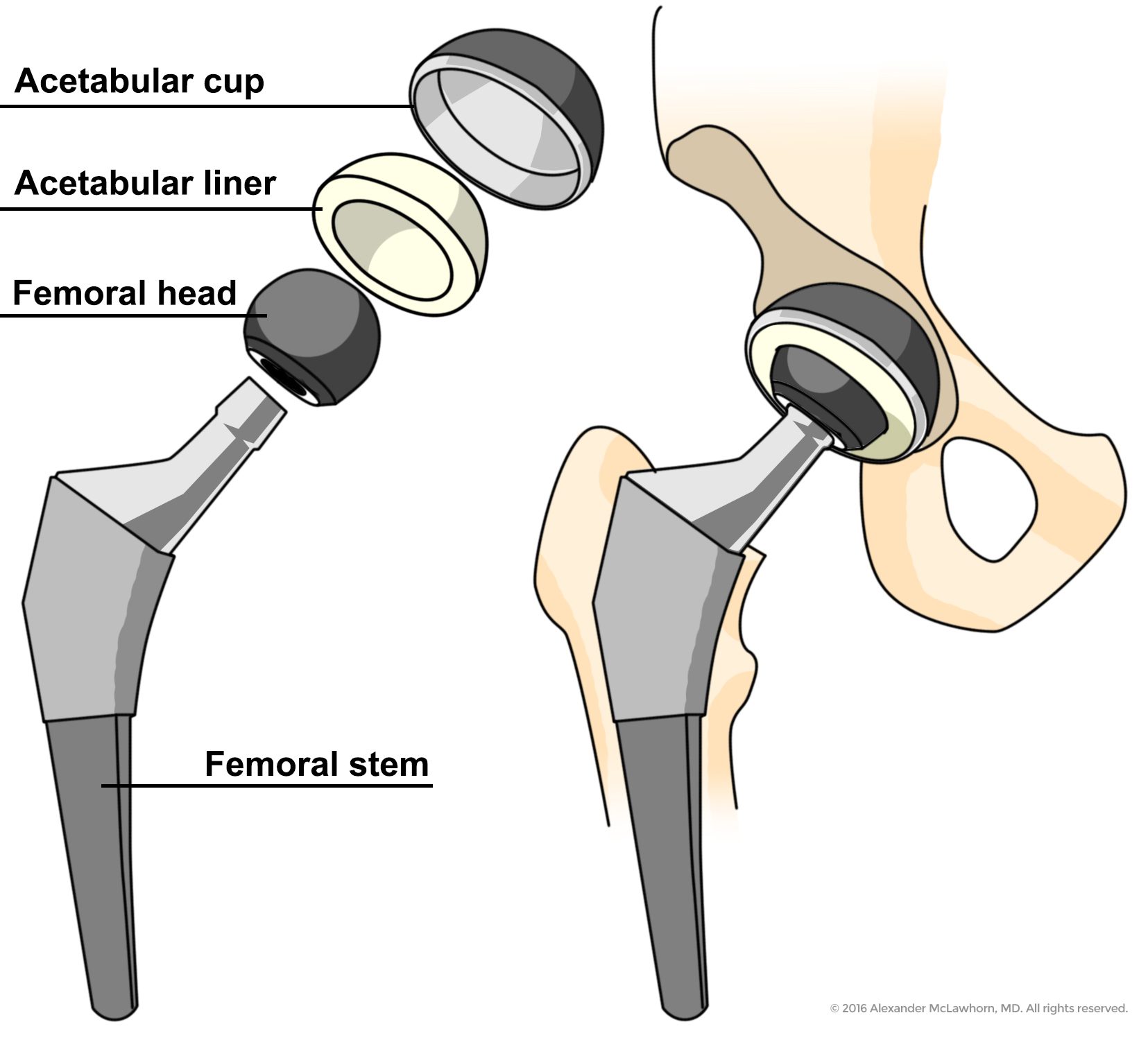
- He will carefully remove the damaged femoral head, then remove the damaged cartilage on the surface of the acetabulum and reshape the socket into a perfect hemisphere.
- Dr. McLawhorn will place a metal socket with a plastic or ceramic liner within the reshaped acetabulum.
- He’ll place a metal stem down the hollowed center of the femur, with a metal or ceramic ball on top of the stem.
- The new ball moves inside the socket liner, providing very low-friction motion.
- Finally, he will close the soft tissues over the hip joint.
What Materials Are Total Hip Replacements Made Of?
Dr. McLawhorn knows hip implants aren’t "one size fits all." He takes the time to select the optimal implant design and materials for each patient, considering their expectations, preferences, and bone size, shape, and quality. The materials used in hip implants can include:
- Acetabulum or “cup”: Titanium or cobalt chrome
- Cup liner: Highly cross-linked polyethylene (plastic) or ceramic
- Femoral head or “ball”: Cobalt chrome, ceramic, or ceramicized metal
- Femoral stem: Titanium or cobalt chrome
- Fixation to the bone: Uncemented or cemented (PMMA)
We typically use uncemented cups and stems with a special coating that allows your bone to grow onto or into the implant. This integration helps your bone and the implant share the load of your body weight. For patients with very poor bone quality, such as those with severe osteoporosis, cemented femoral stems are an excellent option due to their proven track record.
Ceramic components are durable, and it's extremely rare for a ceramic femoral head to fracture. While ceramic liners are used less frequently, they are an option for younger patients who prefer ceramic over plastic and understand the associated risks, such as ceramic liner fracture and/or squeaking.
Which Surgical Approach Does Dr. McLawhorn Use?
The topic of surgical approaches to the hip has become popular in the news media, and it can be confusing for patients.
There are many approaches to the hip joint — from the front (anterior), from the side (lateral or anterolateral), and the back (posterior or posterolateral). All of them have been used for over half a century, although small modifications in surgical techniques have optimized some approaches for hip replacement surgery.
Dr. McLawhorn primarily uses the anterior approach to access the hip joint for total hip replacement surgery. There are many advantages to this approach over alternatives, including less postoperative pain, accelerated recovery, improved range of motion, and, most importantly, less risk of hip dislocation.
Contrary to what many people hear, most patients are candidates for this approach and its benefits. The risks of this surgery in experienced hands are no different than other approaches. In fact, a recent analysis of almost 5,000 THRs performed at the Hospital for Special Surgery showed that the risks of infection, fracture, and other complications were equivalent for anterior and posterior approach THR, and anterior approach THR had a significantly lower risk of dislocation and reoperation compared to posterior approach THR.
Dr. McLawhorn believes that most patients are candidates for anterior approach surgery. Many patients are pleasantly surprised when Dr. McLawhorn recommends the anterior approach THR for them because they've been told they are not candidates for this approach by other surgeons. An important exception for Dr. McLawhorn is excessive soft tissue (pannus) overlying the area where the surgical incision will be made, as this is a risk for surgical site infection. More rarely, the complexity of the joint replacement may dictate a different surgical approach. Some patients may be candidates for a "bikini" style incision with the direct anterior approach, which offers a more discreet scar and improved cosmetics of the scar.
The choice of surgical approach is based upon patient preference, expectations, anatomy, bone quality, and complexity of the hip replacement procedure. Regardless of the surgical approach used, the long-term goals of total hip replacement are the same: eliminate pain, improve function, provide a stable hip, prevent excessive implant wear, and minimize the likelihood of complications.
What Is Direct Anterior Approach Hip Replacement Surgery?

The direct anterior approach has been used for hip replacements since the 1950s, but it didn’t gain popularity in the United States until the early 2000s. Direct anterior hip replacement surgery is less invasive, causes less muscle damage, and affords quicker recovery than other approaches to the hip. These popular perceptions about the approach have made it a more frequently utilized approach for total hip replacement.
The approach is unique because it accesses the hip joint by utilizing a natural space or “plane” between muscles around the hip rather than going through muscle or cutting muscle. Therefore, less muscle damage occurs with this approach, and it is considered soft tissue-sparing surgery. This leads to less pain and a lower likelihood of hip dislocation after the surgery.
During your hip replacement surgery, you’ll lie on your back. We make an incision over the belly of the tensor fascia lata muscle, located in front of your hip. The length of this incision depends on the depth of the fatty tissue and muscle overlying your hip, typically ranging from four to six inches. The goal is to have full access to the top of your thigh bone and the socket, allowing us to place the prosthetic components precisely and accurately.
We retract the muscles in front of your hip to the sides of the incision, exposing and incising the anterior (front) of the hip capsule to access your hip joint. We repair the capsule at the end of the surgery to promote healing.
Anterior Hip Replacement Recovery
After your surgery, you won't need to follow "hip precautions." While certain hip positions might increase the risk of dislocation in the immediate weeks following surgery, these positions are uncommon in most everyday activities. Our goal is to help you return to your daily routine as smoothly and safely as possible.

Understanding the Anterior Approach
Using an anterior approach for hip replacement allows Dr. McLawhorn to make incisions at the front of the hip instead of cutting through the muscles and tendons. This technique also reduces the risk muscle injury during surgery. It is associated with reduced risk of postoperative dislocation of the prosthesis, less pain and faster recovery, compared to posterior approach surgery.
Advantages of Anterior Approach for Hip Replacement
In addition to reducing muscle injury, using an anterior approach also offers patients:
- Shorter recovery period: One of the main advantages of using an anterior approach to hip replacement is a shorter recovery period. Since the muscles and nerves are spared during surgery, you need less time to heal. Patients may also experience less postoperative pain as well.
- Improved stability: Using an anterior approach also provides a visual field for more accurate placement of the hip prosthetic. This can improve hip stability and possibly lower the risk of hip dislocation.
- Fewer postoperative restrictions: With fewer incisions and preservation of muscles and tendons, patients may also have fewer postoperative restrictions. Patients may have a better range of motion in their hip and also be able to bear weight sooner when compared to patients who underwent hip replacement via a posterior approach.
What Is Posterior Hip Replacement Surgery?
Popular media has labeled posterior hip replacement surgery as “traditional” hip replacement surgery. Historically, the posterior approach was the dominant approach in the US for hip replacement because of its ease and reproducibility.
During your posterior approach hip replacement surgery, we will place you on your side with your surgical hip facing up towards the ceiling. Dr. McLawhorn will make an incision over your buttock, just behind the top of your thigh bone. This allows us to access the top of your thigh bone and the socket to place the prosthetic components.
He’ll split part of the large gluteus maximus muscle and release the small tendons and muscles attached to the back of your hip joint. He’ll then open the posterior hip capsule to access the hip joint and replace it, and then repair it during the closing steps of the procedure. Any tendons released during the procedure are likewise repaired, after the prosthetic is placed.
Posterior Hip Replacement Recovery
In the first four to six weeks after posterior approach hip surgery, we may ask you to follow “hip precautions,” which entails not performing deep hip flexion, crossing the operated leg across your body (adduction), or internally rotating the hip (generally, positioning the leg so that you see its outer, or lateral, aspect). Combining these motions is the most dangerous in the first 12 weeks after surgery and can cause a hip dislocation. Following the prescribed precautions allows the repaired soft tissues to heal and will give you a stable hip that is unlikely to dislocate in the future. Dr. McLawhorn has shown that the repair of the capsule and tendons is durable for years after surgery.
While the posterior approach historically had a high dislocation rate compared to other approaches, soft tissue repair, precise component placement with robotics, and modern implant designs do lower the dislocation risk. In fact, robotic assisted total hip replacement is associated with approximately 50% reduction in dislocation risk compared to traditional, manual prosthetic placement.
How Does The Anterior Approach Compare To The Posterior Approach?
The primary differences between the anterior approach and posterior approach are:
- The risk of dislocation (lower risk for the anterior approach)
- Easier, faster recovery for anterior approach
- Less postoperative pain for anterior approach
- Temporary numbness along the thigh after the anterior approach.
- Higher risk of wound healing issues, particularly in older, female patients with elevated body mass index, with anterior approach
| Functional recovery? | No precautions, slightly faster | Precautions, slightly slower |
| Dislocation risk? | Significantly lower | Higher |
| Blood loss? | Equivalent | Equivalent |
| Risk of complication during surgery? | Low, no significant differences | Low, no significant differences |
| Level of postoperative pain? | Lower | Higher |
| Likelihood of major nerve injury? | No difference, very low | No difference, very low |
| Likelihood of minor nerve injury or dysfunction? | Higher, usually affecting the “lateral femoral cutaneous nerve”, and resolves in the majority of instances | Very low |
| Suitability for all patients? | May be less suitable for obese patients or patients with very complex hip anatomy | Suitable for all patients |
| Special table required? | Not required, but often used | Not required, but often used |
| Minimally invasive? | Yes | Yes |
| Difference in long-term outcome? | No, other than risk of dislocation (lower) | No, other than risk of dislocation (higher) |
| Use of X-ray during surgery? | Frequently; Easy to use | Almost never; Less easy to use |
| Able to use advanced technology, like computer-assisted or robot-assisted surgery? | Yes | Yes |
Considerations of Each Surgical Approach
Both surgical approaches provide patients with a variety of benefits. However, it’s equally important to understand that not every patient is suitable for an anterior or posterior approach.
One of the most significant factors in successfully using an anterior approach is the surgeon’s level of expertise. Surgeons specializing in anterior approach hip replacements, like Dr. McLawhorn, understand that patient anatomy is equally important.
Some patients may not have the right bone structure to use an anterior approach. In those cases, a posterior approach may be the better alternative. Dr. McLawhorn will discuss all of your surgical options in your consultation so you understand the pros and cons of each approach.
Frequently Asked Questions
How Do I Decide When I Need a Hip Replacement?
Choosing to have hip replacement surgery is a personal decision that you can make with the guidance of Dr. McLawhorn. Your preference for surgery, lifestyle demands, and expectations for outcomes after surgery aid the decision-making process and will guide your choice between nonsurgical care and hip surgery.
In general, when hip pain begins to interfere with your daily life, prevents you from participating in your recreational activities, wakes you from sleep, and/or requires prescription pain medication, hip replacement surgery is a consideration.
What Can I Expect After Total Hip Replacement?
Immediately after surgery, you can walk on your hip replacement. A walker, crutches, or cane may be used for several weeks if needed. Dr. McLawhorn recommends following posterior hip precautions (no hip flexion greater than 90 degrees, no crossing of the operated leg over the body, and no internal rotation) for six weeks if you have posterior approach surgery. Follow these general guidelines during that time:
- Sit in a high chair or use two pillows on a standard chair
- Use a chair with armrests
- Keep your knees apart when getting up from a seated position
- Use a raised toilet seat
- Use a pillow between your legs when sleeping at night
He advises anterior hip precautions (no excessive hip extension and no excessive hip external rotation) for six weeks after anterior approach surgery. Depending on the demands of your job, you may return to work within two weeks of surgery. You should be able to return to normal activities, including heavy labor, after 3 months and return to impact sports six months after surgery.
Dr. McLawhorn recommends routine follow-ups with all his hip replacement patients. In general, we like to evaluate patients at six weeks, one year, five years, and then every five years after surgery. We’ll perform a clinical examination and X-rays at each of these visits.
How Long Will a Total Hip Replacement Last?
Current data suggests that the lifelong risk of revision or re-do surgery after contemporary total hip replacement is less than 5%. With continued improvements in joint implant technology and surgical techniques, these numbers may improve.
What Is the 90% Rule With Hip Replacement?
The 90% rule with hip replacement refers to the expectation that patients will achieve 90% of their maximum improvement in hip function and pain relief within the first three months after surgery. This means that the majority of recovery and improvement occurs relatively quickly, with the remaining 10% of progress taking place over the following months. It highlights the rapid benefits of the surgery while also setting realistic expectations for the full recovery period.
What Is the Ideal Weight for Hip Surgery?
There is no specific "ideal" weight for hip surgery, but maintaining a healthy weight can significantly impact the outcome and recovery process. Excess weight can put additional stress on the new hip joint, potentially affecting its longevity and increasing the risk of complications. Surgeons often recommend that patients achieve a body mass index (BMI) within a healthy range before having hip replacement surgery to optimize results and reduce risks. Dr. McLawhorn recommends BMI of 40 or less for total hip replacement. If your BMI is over 35, anterior approach surgery is offered less frequently. Patients with BMI over 45 requires consultation with a weight management specialist prior to surgical consideration.
Is It Possible to Wait Too Long for Total Hip Replacement Surgery?
Yes, waiting too long for total hip replacement surgery can lead to worsening joint damage, increased pain, and decreased mobility. Delaying surgery might also cause secondary issues, such as muscle atrophy and decreased overall physical condition. Sometimes the bone stock around the hip becomes compromised such that placement of the prosthetic parts becomes more technically challenging. These issues can complicate surgery, recovery and reduce the effectiveness of the procedure. Consult with Dr. McLawhorn to determine the optimal timing for surgery based on individual health and the progression of hip joint damage.
What are the signs I need a total hip replacement?
Common signs that you may need a total hip replacement include chronic hip pain that interferes with daily activities, difficulty walking or standing, pain that persists even at rest or during sleep, reduced range of motion, stiffness in the hip joint, and ineffective relief from pain medications or other treatments. Severe arthritis or hip damage confirmed by X-rays may also indicate the need for surgery.
How do I prepare for a total hip replacement surgery?
To prepare, you should discuss any medications with your surgeon, as some may need to be stopped before surgery. You may be advised to lose weight if you're overweight to reduce stress on the new joint. Preparing your home for a safer recovery (e.g., removing tripping hazards, arranging for help, and installing safety bars) is essential. You might also be instructed to do pre-surgical exercises to strengthen the surrounding muscles. Strengthening of the hip abductor muscles and core muscles is recommended in particular.
Will I need physical therapy after surgery?
Not necessarily. Walking is crucial for recovery after a total hip replacement and the primary "therapy" needed for recovery. It helps restore mobility, strengthen the muscles around the hip, and improve flexibility and balance. Dr. McLawhorn typically advises avoiding outpatient physical therapy for the first 6 weeks after THR. If there is patient desire or specific deficit of concern at 6 weeks postoperatively, then Dr. McLawhorn will make a referral for formal physical therapy. The majority of patients can return to low impact exercise and gym at 6 weeks for self-direct exercise, and they will not require formal physical therapy.
What are the potential risks and complications of total hip replacement?
Potential risks and complications may include infection, blood clots, implant dislocation, nerve or blood vessel injury, differences in leg length, implant loosening or wear over time, and reactions to anesthesia. While these risks are relatively low, following your surgeon's instructions is essential to minimize them.
Will I need to use a walker or cane after the surgery?
Yes, you will likely use a walker, cane, or crutches for a few weeks after the surgery to assist with mobility and balance as you regain strength in your hip.
Is there an age limit for having a total hip replacement?
There is no established age limit for hip replacement surgery. It is typically based on the patient's overall health, pain level, mobility, and quality of life. While most hip replacement patients are between 40 and 80 years old, younger or older individuals can still be candidates if they meet the medical criteria.
Will I have a scar after a hip replacement, and how noticeable will it be?
Yes, you will have a scar from the surgery. The scar's size and appearance depend on which surgical technique is used. Minimally invasive procedures may result in smaller scars, while traditional approaches might leave longer ones. Over time, the scar will fade, becoming less noticeable, and scar treatments (creams, gels, or silicone sheets) can further improve its appearance.
What should I do if I experience pain years after my hip replacement surgery?
If you experience pain years after hip replacement, consult your orthopedic surgeon to determine the cause. Pain could indicate issues like implant wear, loosening, infection, or surrounding tissue problems. Early evaluation and intervention can help prevent more severe complications and may involve imaging tests, physical exams, or revision surgery if necessary.
Are There Any Non-Surgical Alternatives to Hip Replacement?
Yes. While total hip replacement is highly effective for relieving pain and restoring mobility, some patients may benefit from non-surgical treatments, especially in the early stages of hip arthritis. These options won’t reverse joint damage but can help manage symptoms for a time.
Non-surgical alternatives include:
- Over-the-counter or prescription anti-inflammatory medications
- Corticosteroid injections to reduce inflammation and pain
- Physical therapy to strengthen the surrounding muscles and improve joint function
- Activity modification and assistive devices, such as a cane or walker
If your hip pain is manageable with these approaches, surgery may not be necessary yet. However, if pain continues to interfere with your life despite conservative care, a total hip replacement may be the next step.
What Activities Should I Avoid After a Total Hip Replacement?
Most patients can return to a full and active lifestyle after total hip replacement, including walking, biking, swimming, hiking, and golf. However, there are a few activities that are best avoided to help protect your new joint and prevent premature wear or complications.
We generally advise avoiding:
- High-impact sports like running, basketball, or singles tennis
- Deep squats or lunges that place excessive force on the hip joint
- Repetitive jumping or twisting motions
- Contact sports or activities with a high fall risk
After surgery, Dr. McLawhorn will review your specific goals and advise you on safe ways to stay active long-term. The majority of patients return to low-impact activities within six weeks and more demanding ones around three to six months postoperatively.
What Should I Expect Regarding Cost and Insurance Coverage for a Hip Replacement?
Costs for total hip replacement can vary depending on your insurance plan, provider network, and any additional care you may need before or after surgery. Most commercial insurance plans and Medicare cover total hip replacement if it’s deemed medically necessary.
Our team will help you navigate your benefits and obtain prior authorization when required. We'll also provide a cost estimate if you’re paying out-of-pocket or have a high-deductible plan. If you have questions about coverage or billing, we’re here to assist before your procedure so there are no surprises.
Can I Get Both Hips Replaced at the Same Time?
In some cases, yes. This is known as bilateral total hip replacement, where both hips are replaced during a single surgery. It may be considered for patients who have severe arthritis or joint damage in both hips, are in good overall health, and are highly motivated to complete a single recovery period.
However, not all patients are good candidates for same-day bilateral hip replacement. The procedure takes longer, carries higher short-term risks, and requires a more intense recovery. Dr. McLawhorn will assess your health history, activity level, and personal goals before recommending whether a staged (separate surgeries) or simultaneous approach is right for you.
How Should I Prepare My Home for Recovery After Hip Replacement?
Setting up your home in advance can make recovery safer and more comfortable. We recommend a few key steps before your surgery:
- Create a clear walking path: Remove loose rugs, cords, or furniture that could cause tripping.
- Set up a main floor living space: If possible, avoid stairs in the first few days after surgery.
- Raise seating surfaces: Use a high chair, firm cushions, or risers to avoid low seating that’s hard to get up from.
- Support bars or grab rails: Install these in the bathroom and shower area to reduce fall risk.
- Place frequently used items within reach: Keep everyday essentials (phone, medications, water, snacks) at waist height to avoid bending or reaching.
When Can I Drive After Total Hip Replacement?
Most patients can return to driving once they are off narcotic pain medications, can sit comfortably, and have good control of the surgical leg. For most people, this is typically around 2 to 4 weeks after surgery—but it varies depending on whether your right or left hip was replaced and your car’s transmission type.
Dr. McLawhorn will assess your mobility, strength, and reaction time at your post-operative visit and let you know when it’s safe to resume driving. If you’re unsure, we recommend waiting until you can comfortably enter and exit the car, press the brake quickly, and have no pain or stiffness that might interfere with safe driving.
What Should I Expect During My First Few Days After Surgery?
The first few days after surgery focus on pain control, mobility, and home safety. Most patients go home the same day or within 24 hours. You'll begin walking with a walker or crutches right away and be encouraged to move regularly to prevent stiffness and blood clots.
You can expect:
- Mild to moderate soreness around the incision and hip
- Swelling in the thigh and lower leg
- Tiredness as your body begins to heal
- Use of a walker or cane to help with balance
- A gradual return to everyday activities
Keeping up with your walking schedule, following your movement precautions (anterior or posterior), and managing discomfort with prescribed medications will support a smoother recovery.
Regain Your Mobility and Comfort With Expert Hip Care
If you’re suffering from debilitating hip pain or hip arthritis and exploring total hip replacement as a treatment option, seek advice from an orthopedic hip specialist like Dr. McLawhorn. Even if you've been told you're not a candidate for anterior approach THR, you may want another opinion about your treatment.
Dr. Alexander McLawhorn is a hip specialist at the Hospital for Special Surgery, serving patients in New York and Stamford, Connecticut. To learn more, call 203-705-2113 (CT) / 212-606-1065 (NYC) today or schedule an appointment by using the form on this page.

